The Certified - Electronic Fetal Monitoring (EFM)
Passing NCC C-EFM exam ensures for the successful candidate a powerful array of professional and personal benefits. The first and the foremost benefit comes with a global recognition that validates your knowledge and skills, making possible your entry into any organization of your choice.
EFM Exam Dumps
- Exam Code: EFM
- Vendor: NCC
- Certifications: C-EFM
- Exam Name: Certified - Electronic Fetal Monitoring
Why CertAchieve is Better than Standard EFM Dumps
In 2026, NCC uses variable topologies. Basic dumps will fail you.
| Quality Standard | Generic Dump Sites | CertAchieve Premium Prep |
|---|---|---|
| Technical Explanation | None (Answer Key Only) | Step-by-Step Expert Rationales |
| Syllabus Coverage | Often Outdated (v1.0) | 2026 Updated (Latest Syllabus) |
| Scenario Mastery | Blind Memorization | Conceptual Logic & Troubleshooting |
| Instructor Access | No Post-Sale Support | 24/7 Professional Help |
Customers Passed Exams
10
Success backed by proven exam prep tools
Questions Came Word for Word
93%
Real exam match rate reported by verified users
Average Score in Real Testing Centre
94%
Consistently high performance across certifications
Study Time Saved With CertAchieve
60%
Efficient prep that reduces study hours significantly
NCC EFM Exam Domains Q&A
Certified instructors verify every question for 100% accuracy, providing detailed, step-by-step explanations for each.
Question 1
NCC EFM
QUESTION DESCRIPTION:
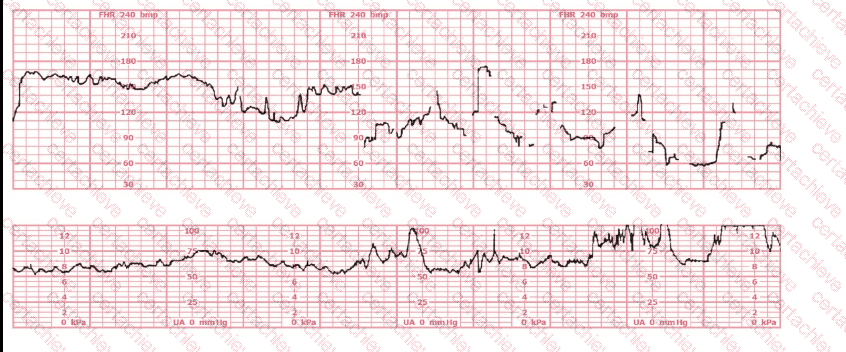
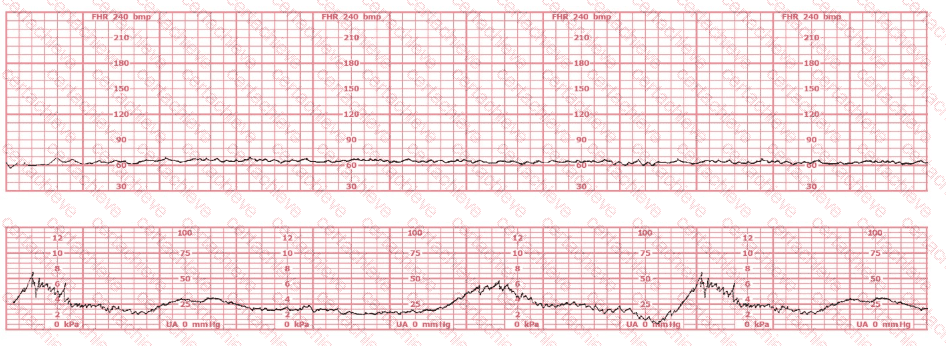
This is a fetal heart rate tracing of a multiparous woman whose cervix is 7 cm dilated on admission. The most likely cause for this pattern is:
Correct Answer & Rationale:
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
The tracing shows a clear relationship between uterine activity and fetal heart rate changes :
The uterine activity strip demonstrates very frequent contractions with little resting time between them , exceeding five contractions in 10 minutes , averaged over a 30-minute window.
NCC and NICHD define tachysystole as “more than 5 contractions in 10 minutes, averaged over 30 minutes, regardless of whether the labor is spontaneous or stimulated.”
As uterine activity intensifies and becomes excessively frequent, the fetal heart rate strip begins to show:
Progressive decrease in baseline
Recurrent decelerations with gradual onset and recovery
Reduced variability in the latter portion of the strip
This pattern is consistent with uteroplacental insufficiency caused by excessive uterine activity (tachysystole). NCC and AWHONN emphasize that tachysystole can result in decreased uterine blood flow and fetal oxygenation, leading to late or prolonged decelerations and eventual bradycardia if not corrected.
Why the other options are less likely:
A. Placental abruption Typically associated with maternal symptoms (pain, vaginal bleeding, firm/boardlike uterus) and often a sustained increase in resting tone or a hypertonic contraction , not simply very frequent contractions. These maternal findings are not described in the vignette.
B. Rapid fetal descent Usually causes variable or early decelerations related to head compression, but the tocodynamometer would not necessarily show this degree of contraction frequency. The lower strip here clearly highlights excessive contractions as the primary problem.
Thus, the tracing’s FHR abnormalities are best explained by tachysystole , making C. Tachysystole the most appropriate answer.
[References:NCC C-EFM Candidate Guide (2025); NCC Content Outline – Pattern Recognition and Intervention; NICHD Three-Tier FHR Interpretation System; AWHONN Fetal Heart Monitoring Principles & Practices; Miller’s Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal–Fetal Medicine., , ]
Question 2
NCC EFM
QUESTION DESCRIPTION:
A fetal heart rate pattern characteristic of fetal neurological injury and impending intrapartum fetal demise is:
Correct Answer & Rationale:
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
A wandering baseline is:
A slow, fluctuating baseline
Low amplitude
No variability
No accelerations
Indicative of severe fetal neurologic injury and terminal fetal status
NCC and AWHONN describe wandering baseline as a preterminal pattern .
Why the other answers are wrong:
A. Marked variability → often transient and not associated with demise.
B. Recurrent lates → concerning but not a neurological-injury pattern unless variability absent.
Correct answer: C. Wandering baseline .
[References:NCC Pattern Recognition; AWHONN FHMPP; Menihan; Simpson & Creehan., ]
Question 3
NCC EFM
QUESTION DESCRIPTION:
The main reason intrauterine pressure catheters are placed is to:
Correct Answer & Rationale:
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
Intrauterine pressure catheters (IUPCs) are an internal uterine activity monitoring device used when external tocodynamometry does not provide adequate assessment of contraction strength or frequency . According to NCC, AWHONN, Miller, and Menihan, the primary indication for placing an IUPC is to obtain accurate, quantitative measurement of uterine activity .
Purpose of IUPC (per NCC and AWHONN):
Measures exact intrauterine pressure in mmHg
Calculates Montevideo units (MVUs) to evaluate adequacy of labor
Clearly differentiates:
Frequency
Duration
Strength (intensity)
Resting tone
NCC explicitly lists the primary purpose as:
“Accurate assessment of uterine contraction pattern and intensity.”
Why the other options are incorrect:
A. Define the quality of the fetal baseline – Incorrect
Fetal heart rate (FHR) baseline quality is determined by fetal ECG or FSE , not IUPC.
IUPCs monitor the uterus, not the fetal cardiac signal.
C. Rule out artifact – Incorrect
While an IUPC can reduce artifact from the toco, this is not its primary purpose .
Artifact is more commonly an issue with external FHR monitoring , corrected by repositioning or placing a fetal scalp electrode—not by using an IUPC.
Correct Answer:
B. Determine the contraction pattern
This aligns directly with NCC’s Electronic Monitoring Equipment domain: IUPCs provide the most accurate and reliable measurement of uterine activity when external monitoring is inadequate.
[References:NCC C-EFM Candidate Guide (2025); NCC Content Outline; AWHONN Fetal Heart Monitoring Principles & Practices; Miller’s Fetal Monitoring Pocket Guide; Menihan Electronic Fetal Monitoring; Simpson & Creehan Perinatal Nursing; Creasy & Resnik Maternal–Fetal Medicine., ]
Question 4
NCC EFM
QUESTION DESCRIPTION:
The baseline fetal heart rate in this tracing is:
Correct Answer & Rationale:
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
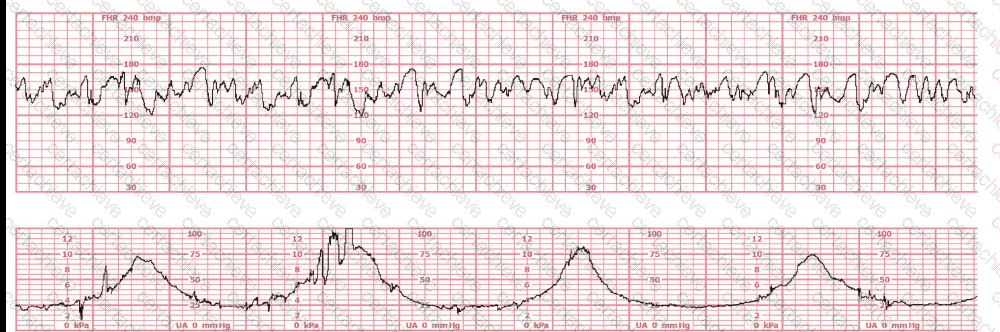
On the tracing:
FHR consistently ranges 170–185 bpm .
Variability remains present, confirming adequate signal.
This pattern persists for the required minimum 10-minute baseline window .
NICHD/NCC define fetal tachycardia as:
Baseline > 160 bpm for at least 10 minutes
Because the FHR is well above 160 for the whole reviewable period, the baseline is tachycardic .
Why the other answers are incorrect:
A. 155 bpm — Too low; FHR visually averages well above this.
B. Indeterminate — Not applicable; variability is clear and the tracing meets the ≥10-minute rule.
Correct answer: C. Tachycardia
[References:NICHD Definitions; NCC C-EFM Candidate Guide; AWHONN; Miller; Menihan., , ]
Question 5
NCC EFM
QUESTION DESCRIPTION:
Sustained fetal supraventricular tachycardia that goes untreated is most likely to result in:
Correct Answer & Rationale:
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
Sustained fetal supraventricular tachycardia (SVT) often produces heart rates > 200–240 bpm , causing:
Poor ventricular filling
Decreased stroke volume
Reduced cardiac output
Congestive heart failure
Progressive fluid accumulation
NCC and AWHONN emphasize that untreated SVT leads to hydrops fetalis , characterized by:
Ascites
Pleural effusion
Pericardial effusion
Skin edema
Why the other answers are incorrect:
A. Fetal anemia — Causes tachycardia but is not caused by SVT.
C. Neonatal pacemaker — Pacemakers treat heart block , not SVT.
Correct answer: B. Hydrops fetalis
[References:NCC C-EFM Candidate Guide; AWHONN Principles & Practices; Simpson & Creehan; Creasy & Resnik Maternal–Fetal Medicine., ]
Question 6
NCC EFM
QUESTION DESCRIPTION:
A fetal heart rate pattern shows no accelerations or decelerations. It would be interpreted as a Category II pattern if it occurred with:
Correct Answer & Rationale:
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NICHD Category II includes:
Minimal variability
Marked variability
Absent accelerations without recurrent decelerations
Indeterminate baseline characteristics
A tracing with no accelerations and no decelerations becomes Category II if paired with marked variability , because marked variability indicates potential stress.
Why other answers are wrong:
A. FHR 110 bpm → normal baseline if variability normal.
B. Sinusoidal pattern → Category III, not Category II.
Correct answer: Marked variability .
[References:NCC Candidate Guide; NICHD FHR Definitions; AWHONN FHMPP; Menihan., ]
Question 7
NCC EFM
QUESTION DESCRIPTION:
The success of interventions to treat fetal hypoxia first depends on:
Correct Answer & Rationale:
Answer: C
Explanation:
Comprehensive and Detailed Explanation From NCC-Aligned Sources:
NCC/AWHONN emphasize that the primary goal of intrauterine resuscitation is to:
Optimize uteroplacental blood flow, which restores fetal oxygen delivery.
Key measures include:
Maternal repositioning (lateral)
Reducing tachysystole
IV fluid bolus
Correcting maternal hypotension
Stopping oxytocin
Treating underlying causes
Improving maternal oxygenation is supportive, but improving uteroplacental perfusion is the critical first determinant of resuscitation success.
Why the other answers are not first priority:
A. Oxygen — optional and no longer universally recommended unless maternal hypoxemia exists.
B. Minimizing uterine activity — essential, but still secondary to restoring perfusion.
Correct answer: C. Optimizing uteroplacental blood flow
[References:NCC Pattern Recognition & Intervention Domain; AWHONN FHMPP; Menihan; Simpson & Creehan., ]
Question 8
NCC EFM
QUESTION DESCRIPTION:
The factor that differentiates a prolonged deceleration from bradycardia is:
Correct Answer & Rationale:
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract–Based NCC C-EFM References:
NICHD/NCC definitions:
Prolonged deceleration: decrease in FHR ≥15 bpm lasting 2 to 10 minutes
Bradycardia: baseline FHR < 110 bpm lasting ≥10 minutes
The differentiating factor is duration , not rate and not contraction relationship.
Before 10 minutes → prolonged deceleration
At or beyond 10 minutes → new baseline → bradycardia
Thus, the factor that differentiates the two is length of time it lasts .
[References:NICHD FHR Definitions; NCC C-EFM Candidate Guide; AWHONN; Miller; Menihan., ]
Question 9
NCC EFM
QUESTION DESCRIPTION:
(Full question statement)
The fetal heart rate tracing shown is obtained upon the woman ' s admission to labor and delivery. This tracing is most consistent with what maternal condition?
Correct Answer & Rationale:
Answer: B
Explanation:
Comprehensive and Detailed Explanation From Exact Extract (NCC C-EFM sources: AWHONN, Miller’s Pocket Guide, Menihan, Simpson, Creasy & Resnik, 2025 Candidate Guide)
The tracing displays baseline fetal bradycardia , with a rate near 100 bpm , minimal variability, and preserved periodic response. According to AWHONN’s Fetal Heart Monitoring Principles & Practices and Menihan’s Electronic Fetal Monitoring , maternal conditions that reduce oxygen-carrying capacity —including maternal anemia —can lead to lower fetal oxygen delivery , prompting a fetal compensatory bradycardic baseline.
Creasy & Resnik’s Maternal-Fetal Medicine notes that sickle cell anemia decreases maternal hemoglobin function even when maternal vital signs appear stable , reducing uteroplacental oxygen transport. Fetuses of mothers with sickling disorders may demonstrate lower resting fetal heart rates due to chronic mild hypoxemia.
Conversely, Eisenmenger’s syndrome is associated with severe maternal cyanosis and high fetal mortality , often producing late decelerations and growth restriction rather than mild bradycardia. Systemic lupus erythematosus (SLE) is commonly associated with heart block (especially with anti-Ro/SSA antibodies), which is not displayed here, as true heart block presents with a fixed atrial–ventricular dissociation and FHR < 60 bpm.
Thus, based on fetal physiology and maternal disease correlations taught in NCC-recommended sources, the tracing is most consistent with maternal sickle cell anemia .
Question 10
NCC EFM
QUESTION DESCRIPTION:
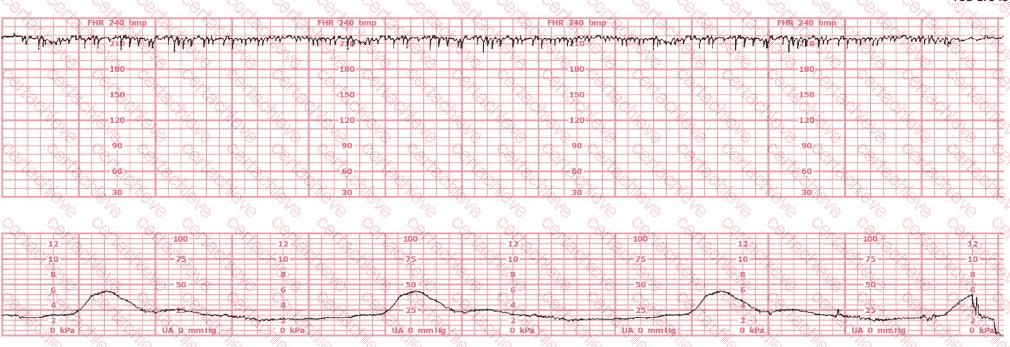
The fetal heart rate tracing shown is consistent with
Correct Answer & Rationale:
Answer: C
Explanation:
Comprehensive and Detailed Explanation From Exact Extract NCC-Recommended Sources
The tracing demonstrates a very rapid, highly regular baseline fetal heart rate with minimal beat-to-beat variability—characteristic of fetal supraventricular tachycardia (SVT) . NCC-recommended references, including AWHONN’s Fetal Heart Monitoring Principles & Practices , Menihan’s Electronic Fetal Monitoring: Concepts and Applications , Simpson & Creehan’s Perinatal Nursing , and Creasy & Resnik’s Maternal-Fetal Medicine all describe fetal SVT as a sustained tachyarrhythmia usually greater than 200 bpm , narrow-complex, and extremely regular in appearance.
AWHONN teaches that SVT appears as a “tight, rapid, uniform baseline with minimal variability.” Menihan states that “SVT may present on EFM as a nearly straight line due to the rapid, consistent rate with micro-oscillations.” This differs significantly from artifact , which appears disorganized, erratic, and inconsistent in amplitude. Additionally, “half-counting” is a Doppler misinterpretation that records half of an extremely fast fetal rate , usually resulting in a falsely lower heart rate—not the very rapid tracing shown here.
Creasy & Resnik emphasize that SVT is the most common pathological fetal arrhythmia and can lead to fetal compromise if prolonged, making accurate recognition essential. Miller’s Pocket Guide to Fetal Monitoring also identifies SVT as a pattern with a “smooth, fast rhythm lacking normal variability.”
All authoritative NCC-recommended references support that this EFM pattern is consistent with fetal SVT , not artifact or half-counting.
[References:, AWHONN – Fetal Heart Monitoring Principles & PracticesMenihan – Electronic Fetal MonitoringSimpson & Creehan – Perinatal NursingCreasy & Resnik – Maternal-Fetal MedicineMiller’s Pocket Guide to Fetal Monitoring, , ]

Verified by Certified Instructors
This NCC EFM study pack was audited and verified on August 9, 2026 by Eric Huntington,. We ensure every technical rationale aligns with real-world enterprise standards.
A Stepping Stone for Enhanced Career Opportunities
Your profile having C-EFM certification significantly enhances your credibility and marketability in all corners of the world. The best part is that your formal recognition pays you in terms of tangible career advancement. It helps you perform your desired job roles accompanied by a substantial increase in your regular income. Beyond the resume, your expertise imparts you confidence to act as a dependable professional to solve real-world business challenges.
Your success in NCC EFM certification exam makes your visible and relevant in the fast-evolving tech landscape. It proves a lifelong investment in your career that give you not only a competitive advantage over your non-certified peers but also makes you eligible for a further relevant exams in your domain.
What You Need to Ace NCC Exam EFM
Achieving success in the EFM NCC exam requires a blending of clear understanding of all the exam topics, practical skills, and practice of the actual format. There's no room for cramming information, memorizing facts or dependence on a few significant exam topics. It means your readiness for exam needs you develop a comprehensive grasp on the syllabus that includes theoretical as well as practical command.
Here is a comprehensive strategy layout to secure peak performance in EFM certification exam:
- Develop a rock-solid theoretical clarity of the exam topics
- Begin with easier and more familiar topics of the exam syllabus
- Make sure your command on the fundamental concepts
- Focus your attention to understand why that matters
- Ensure hands-on practice as the exam tests your ability to apply knowledge
- Develop a study routine managing time because it can be a major time-sink if you are slow
- Find out a comprehensive and streamlined study resource for your help
Ensuring Outstanding Results in Exam EFM!
In the backdrop of the above prep strategy for EFM NCC exam, your primary need is to find out a comprehensive study resource. It could otherwise be a daunting task to achieve exam success. The most important factor that must be kep in mind is make sure your reliance on a one particular resource instead of depending on multiple sources. It should be an all-inclusive resource that ensures conceptual explanations, hands-on practical exercises, and realistic assessment tools.
Certachieve: A Reliable All-inclusive Study Resource
Certachieve offers multiple study tools to do thorough and rewarding EFM exam prep. Here's an overview of Certachieve's toolkit:
NCC EFM PDF Study Guide
This premium guide contains a number of NCC EFM exam questions and answers that give you a full coverage of the exam syllabus in easy language. The information provided efficiently guides the candidate's focus to the most critical topics. The supportive explanations and examples build both the knowledge and the practical confidence of the exam candidates required to confidently pass the exam. The demo of NCC EFM study guide pdf free download is also available to examine the contents and quality of the study material.
NCC EFM Practice Exams
Practicing the exam EFM questions is one of the essential requirements of your exam preparation. To help you with this important task, Certachieve introduces NCC EFM Testing Engine to simulate multiple real exam-like tests. They are of enormous value for developing your grasp and understanding your strengths and weaknesses in exam preparation and make up deficiencies in time.
These comprehensive materials are engineered to streamline your preparation process, providing a direct and efficient path to mastering the exam's requirements.
NCC EFM exam dumps
These realistic dumps include the most significant questions that may be the part of your upcoming exam. Learning EFM exam dumps can increase not only your chances of success but can also award you an outstanding score.
Top Exams & Certification Providers
New & Trending
- New Released Exams
- Related Exam
- Hot Vendor